WHAT IS AN ANAL ABSCESS OR FISTULA?
An anal abscess is an infected cavity filled with pus found near the anus or rectum. Ninety percent of abscesses are the result of an acute infection in the internal glands of the anus. Occasionally, bacteria, fecal material or foreign matter can clog an anal gland and tunnel into the tissue around the anus or rectum, where it may then collect in a cavity called an abscess.
An anal fistula (also commonly called fistula-in-ano) is frequently the result of a previous or current anal abscess. This occurs in up to 40% of patients with abscesses. A fistula is an epithelialized tunnel that connects a clogged gland inside the anal canal to the outside skin.
CLASSIFICATION
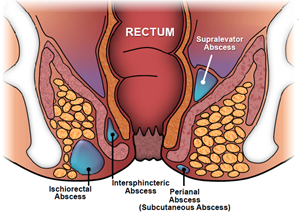 Anal abscesses are classified by their location in relation to the structures comprising and surrounding the anus and rectum: perianal, ischioanal, intersphincteric and supralevator. The perianal area is the most common and the supralevator the least common. If any of these particular types of abscess spreads partially circumferentially around the anus or the rectum, it is termed a horseshoe abscess.
Anal abscesses are classified by their location in relation to the structures comprising and surrounding the anus and rectum: perianal, ischioanal, intersphincteric and supralevator. The perianal area is the most common and the supralevator the least common. If any of these particular types of abscess spreads partially circumferentially around the anus or the rectum, it is termed a horseshoe abscess.
Fistulas are classified by their relationship to parts of the anal sphincter complex (the muscles that allow us 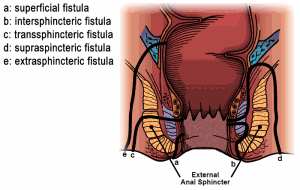 to control our stool). They are classified as intersphincteric, transsphincteric, suprasphincteric and extrasphincteric. The intersphincteric is the most common and the extrasphincteric is the least common. These classifications are important in helping the surgeon make treatment decisions.
to control our stool). They are classified as intersphincteric, transsphincteric, suprasphincteric and extrasphincteric. The intersphincteric is the most common and the extrasphincteric is the least common. These classifications are important in helping the surgeon make treatment decisions.
SYMPTOMS
Anorectal pain, swelling, perianal cellulitis (redness of the skin) and fever are the most common symptoms of an abscess. Occasionally, rectal bleeding or urinary symptoms, such as trouble initiating a urinary stream or painful urination, may be present.
Patients with fistulas commonly have a history of a previously drained anal abscess. Anorectal pain, drainage from the perianal skin, irritation of the perianal skin, and sometimes rectal bleeding, can be presenting symptoms of a fistula-in-ano.
EXAMINATION
A careful history regarding anorectal symptoms and past medical history are necessary, followed by a physical examination. Common findings leading to the diagnosis of a perirectal abscess are fever, redness, swelling and tenderness to palpation. However, while most abscesses are visible on the outside of the skin around the anus, it is important to recognize that there may be no external manifestation of an abscess, other than a complaint of rectal pain or pressure. A digital rectal exam may cause exquisite pain.
When diagnosing an anal fistula, an external opening that drains pus, blood or stool is usually seen on examination. Heaped up tissue at the external opening suggests a well-established fistula. A digital rectal exam may produce pus from the external opening. Some fistulas will close spontaneously and the drainage may be intermittent, making them hard to identify at the time of the office visit. A ‘cord’ or tract can be occasionally palpated from the external opening toward the anal canal indicated where an internal opening of the fistula may be.
USE OF DIAGNOSTIC STUDIES
Most anal abscesses and fistula-in-ano are diagnosed and managed on the basis of clinical findings. Occasionally, additional studies can assist with the diagnosis or delineation of the fistula tract. Today, both traditional two-dimensional and three-dimensional endoanal ultrasound are a very effective manner of diagnosing a deep perirectal abscess, identifying a horseshoe extension of the abscess, and delineating the path of a fistula tract. This may be combined with hydrogen peroxide injection into the fistula tract (via the external opening) to increase accuracy. CT scans can be useful for patients with complicated infections, multiple fistula tracts or with other medical conditions which may present similarly, such as Crohn’s disease. A pelvic MRI has been shown to have accuracy up to 90% for mapping the fistula tract and identifying internal openings.
TREATMENT OF ANAL ABSCESS
The treatment of an abscess is surgical drainage under most circumstances. An incision is made in the skin near the anus to drain the infection. This can be done in a doctor’s office with local anesthetic or in an operating room under deeper anesthesia. Hospitalization and antibiotics may be required for patients prone to more significant infections, such as diabetics or patients with decreased immunity.
Up to 50% of the time after an abscess has been drained, a tunnel (fistula) may persist, connecting the infected anal gland to the external skin. This typically will involve some type of drainage from the external opening. If the opening on the skin heals when a fistula is present, a recurrent abscess may develop. Until the fistula is eliminated, many patients will have recurring cycles of pain, swelling and drainage, with intervening periods of apparent healing.
Antibiotics alone are a poor alternative to drainage of the infection. The routine addition of antibiotics to surgical drainage does not improve healing time or reduce the potential for recurrences in uncomplicated abscesses. There are some conditions in which antibiotics are indicated, such as patients with compromised or altered immunity or in the setting of extensive cellulitis (spreading of infection in the skin). The American Heart Association recommends the use of antibiotics for patients with prosthetic valves, previous bacterial endocarditis, congenital heart disease and heart transplant recipients with valvular pathology. A comprehensive discussion of your past medical history and a physical exam are important to determine if antibiotics are indicated.
TREATMENT OF ANAL FISTULA
Currently, there is no medical treatment available for this problem and surgery is almost always necessary to cure an anal fistula. If the fistula is straightforward (involving minimal sphincter muscle), a fistulotomy may be performed. This procedure involves unroofing the tract, thereby connecting the internal opening within the anal canal to the external opening and creating a groove that will heal from the inside out.
The surgery may be performed at the same time as drainage of an abscess, although most commonly the fistula doesn’t become obvious until weeks after the initial drainage. Fistulotomy is a long-standing treatment with a high success rate (92-97%). This high success rate must be balanced, however with risk of incontinence (ability to control stool) that comes with division of the anal sphincter muscle. Small amount of muscle can usually be safely divided to treat the anal fistula without compromising continence. Therefore, the surgeon must assess whether a fistulotomy is appropriate for a given patient.
In addition to fistulotomy, there are a number of other surgical treatment options for anal fistula which do not involve division of the sphincter muscles. The two most common procedures utilized in these patients are the endoanal advancement flap and the LIFT procedure.
An endoanal advancement flap is a procedure usually reserved for complex fistulas or for patients with an increased potential risk for suffering incontinence from a traditional fistulotomy. In this procedure, the internal opening of the fistula is covered over by healthy, native tissue in an attempt to close the point of origin of the fistula. Recurrence rates have been reported to be up to 50% of cases. Certain conditions, such as Crohn’s disease, malignancy, radiated tissue and previous attempts at repair, and smoking, increase the likelihood of failure. Although the sphincter muscle is not divided in this procedure, mild to moderate incontinence has still been reported.
Another non-sphincter dividing treatment for anal fistula is the LIFT (ligation of the intersphincteric fistula tract) procedure. This procedure involves division of the fistula tract in the space between the internal and external sphincter muscles. This procedure avoids division of the sphincter muscle, and has similar success rate of an endoanal advancement flap.
Most of the operations can be performed on an outpatient basis, but in selected cases, may require hospitalization. Consider identifying a specialist in colon and rectal surgery who will be familiar with a number of potential operations to treat the fistula.
WHAT IS A SETON?
As mentioned above, if a significant amount of sphincter musculature is involved in the fistula tract, a fistulotomy may not be recommended as the initial procedure. Your surgeon may recommend the initial placement of a draining seton. This is often a thin piece of rubber or suture which is placed through the entire fistula tract and the ends of the seton (or drain) are brought together and secured, thereby forming a ring around the anus involving the fistula tract. The seton may be left in place for 8-12 weeks (or indefinitely in selected cases), with the purpose of providing controlled drainage, thereby allowing all the inflammation to subside and form a solid tract of scar along the fistula tract. This is associated with minimal pain and you can still have normal bowel function with a seton in place. Once all the inflammation has resolved, and a mature tract has formed, one may consider all the various surgical options detailed above as staged procedures.
TREATMENT OF FISTULAS IN CROHN’S DISEASE
Fistula-in-ano is very common in Crohn’s disease, which is a chronic inflammatory condition that can affect any part of the gastrointestinal tract. Patients with Crohn’s disease are at increased risk for fecal incontinence because anorectal Crohn’s disease tends to recur and may lead to multiple operations involving the sphincter muscle. It is important to acknowledge that the primary treatment of Crohn’s perianal fistulas is medical, with surgery reserved for treating infection and, occasionally, as a supplement to medical therapy. The treatment should be individualized to the specific patient and incorporate factors that may decrease the potential for fecal incontinence.
WHAT IS THE RECOVERY LIKE FROM SURGERY?
Pain after surgery is controlled with pain medication, fiber, and water. Patients should plan for time at home using sitz baths and avoiding the constipation that can be associated with prescription pain medication. Discuss with your surgeon the specific care and time away from work prior to surgery to prepare yourself for post-operative care.
CAN THE ABSCESS OR FISTULA RECUR?
As previously mentioned, up to 50% of abscesses may re-present as another abscess or as a frank fistula. Despite proper treatment and apparent complete healing, fistulas can potentially recur, with recurrence rates dependent upon the particular surgical technique utilized. Should similar symptoms arise, suggesting recurrence, it is recommended that you find a colon and rectal surgeon to manage your condition.
WHAT IS A COLON AND RECTAL SURGEON?
Colon and rectal surgeons are experts in the surgical and non-surgical treatment of diseases of the colon, rectum and anus. They have completed advanced surgical training in the treatment of these diseases as well as full general surgical training. They are well-versed in the treatment of both benign and malignant diseases of the colon, rectum and anus and are able to perform routine screening examinations and surgically treat conditions if indicated to do so.
DISCLAIMER
The American Society of Colon and Rectal Surgeons is dedicated to ensuring high-quality patient care by advancing the science, prevention and management of disorders and diseases of the colon, rectum and anus. These brochures are inclusive but not prescriptive.
Their purpose is to provide information on diseases and processes, rather than dictate a specific form of treatment. They are intended for the use of all practitioners, health care workers and patients who desire information about the management of the conditions addressed. It should be recognized that these brochures should not be deemed inclusive of all proper methods of care or exclusive of methods of care reasonably directed to obtain the same results. The ultimate judgment regarding the propriety of any specific procedure must be made by the physician in light of all the circumstances presented by the individual patient.